an initiative by SEEK Development
Insight
0 min read
Learning from COVID-19

Written by
Emily Wymer, Sinéad Dwyer
Published on
July 13, 2022
Executive Summary
The COVID-19 crisis revealed serious gaps in health system structures, particularly in disease surveillance capacity and financing worldwide. Momentum for disease surveillance scale-up has increased in the wake of the COVID-19 pandemic and advocates should capitalize on intensified support to encourage donors to fill the gaps.
SEEK Development, with support from the Bill and Melinda Gates Foundation, set out to address the gap in disease surveillance financing knowledge by estimating a baseline level of funding that is currently directed toward disease surveillance systems worldwide. The resulting report presents our best estimate of existing international and domestic funding for disease surveillance.
What we found:
- COVID-19 exposed serious gaps in disease surveillance capacity and financing;
- The COVID-19 pandemic sparked a significant increase in international funding for disease surveillance;
- Disease surveillance funding is mostly disease-specific. Large-scale emergency financing for COVID-19 in recent years supports this trend;
- Current funding needs are far greater than financing; and
- Stakeholders need to act now to ensure adequate disease surveillance financing to respond better to future pandemics and strengthen health systems overall.
Surveillance capacity and financing gaps
Our frontline defense - strong surveillance systems that can rapidly detect emerging infectious diseases and respond to them - was exposed by the COVID-19 pandemic and had serious shortcomings. Lack of diagnostic capacity, limited contact tracing, and fragmented and incomplete data systems prevented rapid identification and containment of SARS-CoV-2. Collected information on the virus was not shared quickly or consistently enough at both the domestic and international levels, limiting individual, government, and multilateral capacity to make well-informed public health decisions.
In addition to pandemic threat response, disease surveillance systems are fundamental to effective national and global health systems. Information collected from disease surveillance systems enables policymakers to allocate scarce resources based on population needs and health burdens, monitor the effectiveness of public health interventions, and identify high-risk population groups or risk factors for disease causation. Policymakers need real-time accurate intelligence to make evidence-based public health decisions to inform disease prevention and control efforts.
Stronger surveillance systems are needed if we are to better respond to the next pandemic threat, tackle emerging global health threats, such as anti-microbial resistance (AMR), and endemic diseases, such as tuberculosis (TB). There has been no transparency on how much money is actually being spent by whom to support disease surveillance in low-resource settings. This report seeks to provide transparency and inform decisions on how funding for disease surveillance can be scaled up and made more efficient.
In 2021, the G20 High Level Independent Panel (HLIP) estimated that an additional US$74 billion in public investment for robust surveillance and detection is needed over the next 5 years to prevent and detect emerging infectious diseases.The panel recommended that US$48 billion (or 66%) of this should come from national budgets, while the remaining US$26 billion should come from international financing.
These estimates provide direction for the global community to improve disease surveillance capacity with a focus on pandemic preparedness, but they do not provide an insight into the current funding situation. Without clarity on current funding trends, it is challenging to translate high-level financing estimates into concrete strategies on how to best mobilize and allocate financing. An enhanced understanding of existing flows is also essential for advocates to champion increased funding for disease surveillance targeted toward areas with the greatest impact.
Be the first to know. Get the latest in development news, right in your inbox.
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.
By clicking Sign Up you're confirming that you agree with our Terms and Conditions .
an initiative by SEEK Development
Disease surveillance systems
Currently, international and domestic funders alike do not have a shared definition of funding for disease surveillance. Their different motivations for investing in disease surveillance result in different perspectives on what constitutes disease surveillance, for example, on whether the cost of diagnostics should or should not be included. In addition, the importance of wider health systems in enabling disease surveillance systems makes it hard to disentangle investments in disease surveillance systems from broader investments in health system strengthening. For example, community health workers (CHW) play an important role in detecting and reporting on health events but disease surveillance is only a small part of their role.
As defined by International Health Regulations (IHR), disease surveillance is, “the systematic ongoing collection, collation and analysis of data for public health purposes and the timely dissemination to those who need to know for public health action”. Within this study, we also incorporated components of the disease surveillance system proposed by the “Not the last pandemic” costing exercise. For the purposes of tracking funding, we grouped the components of a disease surveillance system into the following four functions:
- Foundational surveillance metrics: all ongoing collection, collation, and reporting of foundational health metrics, including mortality, burden of disease, vital statistics, etc.
- Laboratory capacity: all surveillance functions that occur within a laboratory setting, including sequencing, reporting, and analysis, as well as capacity building to enable these functions.
- Programmatic surveillance: all surveillance functions occurring at the health services level, including detection, case reporting, rapid response, notifiable disease surveillance, etc. This includes both disease-specific and non-specific programs.
- Governance, analysis, and decision-making for surveillance: the enabling administrative functions that ensure a well-running surveillance system, including integration and analysis of data, coordination and information exchange, policy making, and decision-making related to surveillance.
International and domestic funding flows
Given there is no common definition of disease surveillance, there is also no systematic tracking of activities or funding that support disease surveillance. Our analysis focused on identifying funding flows from three key categories of international funders - donor governments, multilateral organizations, and philanthropic foundations - for 2019 and 2020 (the first year of the COVID-19 crisis). Given the lack of a comprehensive data source, the analysis made use of a mixed-methods estimation approach, drawing on keyword analysis of OECD CRS datasets on ODA flows, as well as desk research and interviews. Informed by this quantitative and qualitative assessment of the baseline, we then developed recommendations on how financing for disease surveillance can be scaled up and made more efficient.
US$2.3 billion in international funding was related to disease surveillance in 2019
US$2.3 billion in international funding in 2019 was related to disease surveillance, reflecting its enabling function, even before the COVID-19 crisis’ impact on funding priorities.
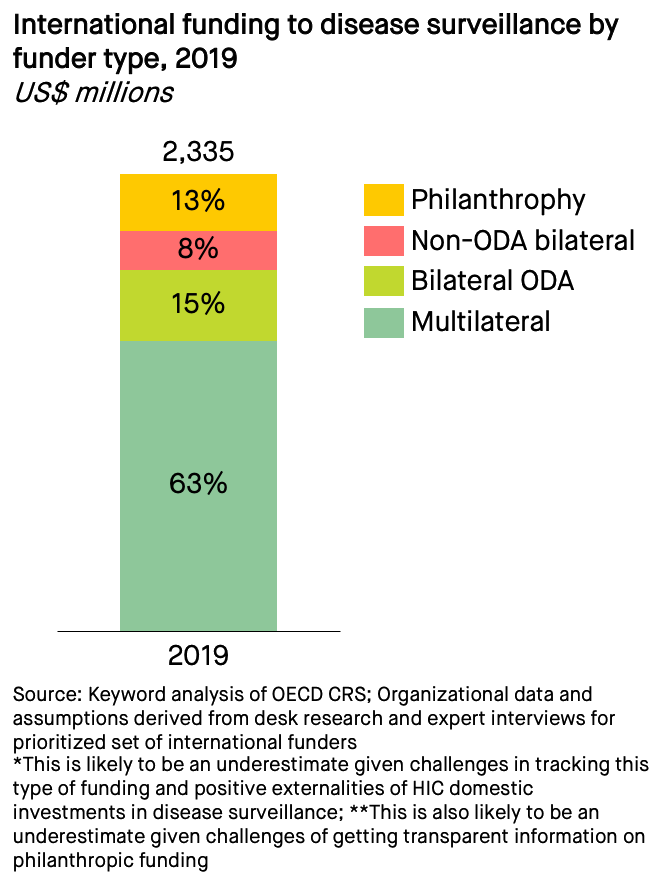
More than half (63%) of identified international funding was channeled through the multilateral system, including as earmarked funding to specific programs and funds managed by multilateral organizations. All the major multilateral organizations in global health (The Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), World Health Organization (WHO), United Nations Children's Fund (UNICEF), World Bank and Gavi, the Vaccine Alliance (Gavi)) funded disease surveillance activities in 2019, reflecting both the complexity and cross-cutting nature of international funding for disease surveillance. The Global Fund, WHO, and World Bank provided more than 80% of total multilateral funding, equivalent to more than half of all international funding.
15% of identified international funding for disease surveillance flowed as bilateral ODA from a small number of donors, notably the US and UK. We sought to determine whether the largest government donors were also using non-development budgets to finance bilateral disease surveillance initiatives. With the notable exception of the US, which has invested internationally using ODA and non-ODA sources since the 1990s to reduce the threat of emerging infectious diseases, we did not identify significant flows that were not already included in bilateral or multilateral ODA estimates.
13% of funding was provided through philanthropic donors in 2019, with the largest contributors being the Bill & Melinda Gates Foundation, Bloomberg Philanthropies, and The Wellcome Trust. The philanthropic funding estimate is conservative, as some philanthropic organizations’ contributions were not quantifiable.
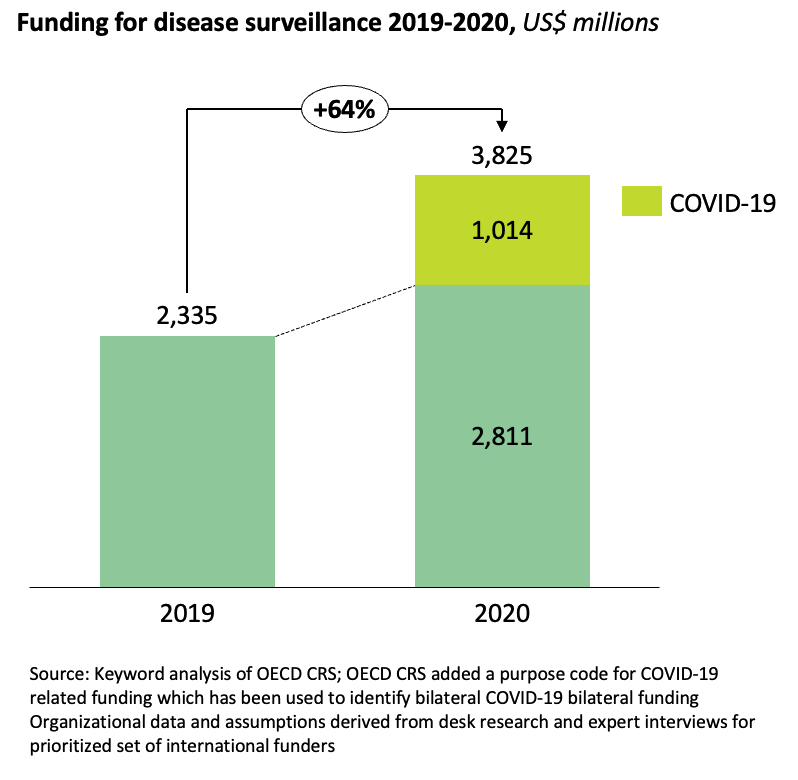
The COVID-19 pandemic sparked a significant increase in international funding for disease surveillance
Funding increased by 64% in 2020 to US$3.8 billion. At least US$1 billion (68%) of the US$1.5 billion increase was directly related to COVID-19 activities. Total ODA only increased by 3.5% in 2020, implying that most of the increased funding for disease surveillance was reallocated from other priorities. Significant amounts of COVID-19-related surge funding came from emergency budgets and went to short-term spending needs; much of this funding is unlikely to contribute to long-term improvements in disease surveillance capacity.
Multilateral funders significantly scaled up funding for disease surveillance in 2020 in response to the COVID-19 crisis. The World Bank increased funding by 169% as a result of significant new programming to support countries to prevent, detect and respond to COVID-19. The Global Fund increased its funding for disease surveillance by 66% in its role as co-convenor of the Access to COVID-19 Accelerator (ACT-A) Diagnostics Pillar, providing additional funding for COVID-19 diagnostic procurement and reinforcing national COVID-19 responses, including case detection, lab capacity, and data collection and analysis; additional resources came from the Global Fund COVID-19 Response Mechanism. WHO increased funding for disease surveillance by 34%, enabling it to provide emergency support for global, regional, and country-level surveillance of COVID-19. WHO’s COVID-19 resources came from the WHO Emergencies Fund, which increased by 141% between 2019 and 2020. Gavi carried out some COVID-19-related disease surveillance in early 2020 before deciding to focus its COVID-19 response exclusively on vaccine equity.
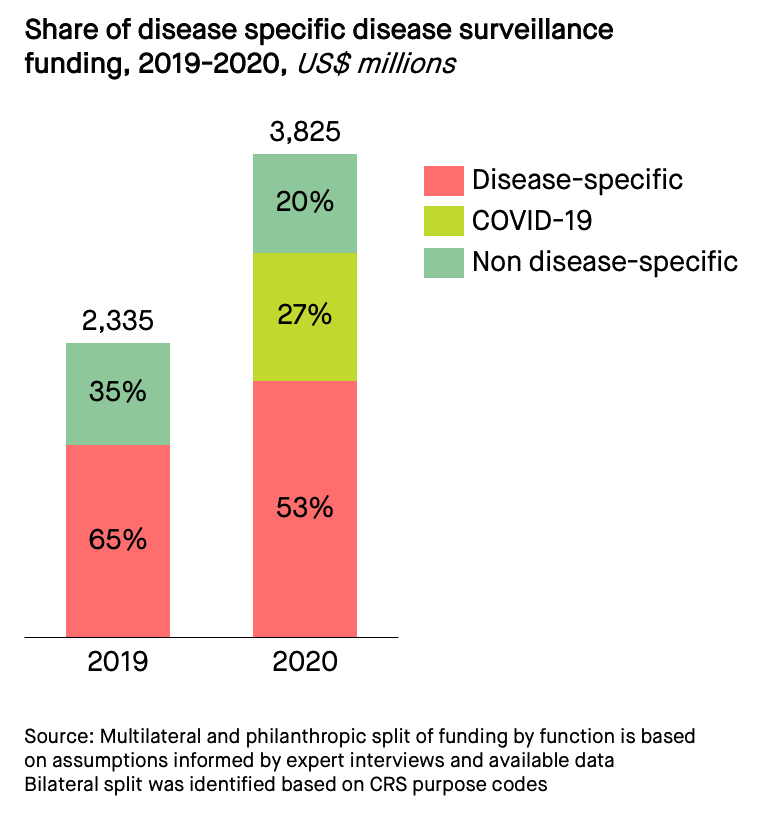
International funding for disease surveillance is mostly disease-specific; scaled-up disease surveillance funding for COVID-19 supports this trend
International funding for disease surveillance is overwhelmingly disease-specific, evidenced by international funders’ rapid scale-up for COVID-19 support in 2020. Significantly less international funding is available for integrated disease surveillance systems or surveillance of often neglected diseases. This trend creates a focus on disease-specific outcomes rather than strengthening integrated disease surveillance systems.
Multilateral funding for disease surveillance is particularly disease-specific. The Global Fund, as the largest funder in 2019, mostly provided disease surveillance funding for its focus diseases, HIV, TB, and malaria. WHO, the second-largest funder in 2019, played a coordinating role, but its funding was still largely disease-specific and responsive. More than one-third (37%) of its estimated funding for disease surveillance comes from the Global Polio Eradication Initiative (GPEI). This funding could contribute to broad disease surveillance systems strengthening but demonstrates that funding allocation is weighted toward polio-related needs.
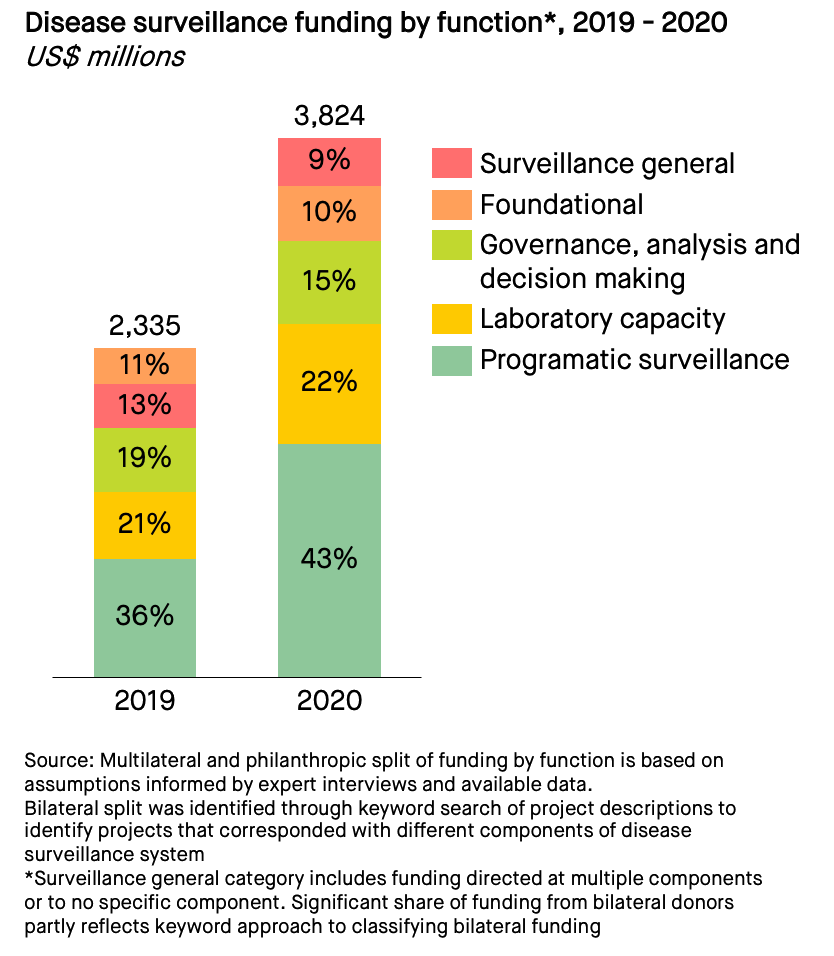
Given the multilaterals’ focus on disease-specific surveillance, it is unsurprising that the largest share of disease surveillance funding in 2019 and 2020 went to programmatic surveillance. In 2020, the volume and share of funding for programmatic surveillance increased as a result of additional COVID-19-related funding. The second-largest share of funding went to laboratory capacity, including from the Global Fund, WHO, and World Bank. Governance, analysis, and decision-making were the third-largest category and came predominantly from WHO and bilateral donors. 11% of disease surveillance funding went to foundational components of disease surveillance in 2019 and came predominantly from the Global Financing Facility (GFF) at The World Bank, UNICEF, and bilateral donors. 13% of funding in 2019 supported ‘surveillance general’, which is indicated for cross-functional projects and non-disease-specific functions; this funding came largely from the World Bank and bilateral donors.
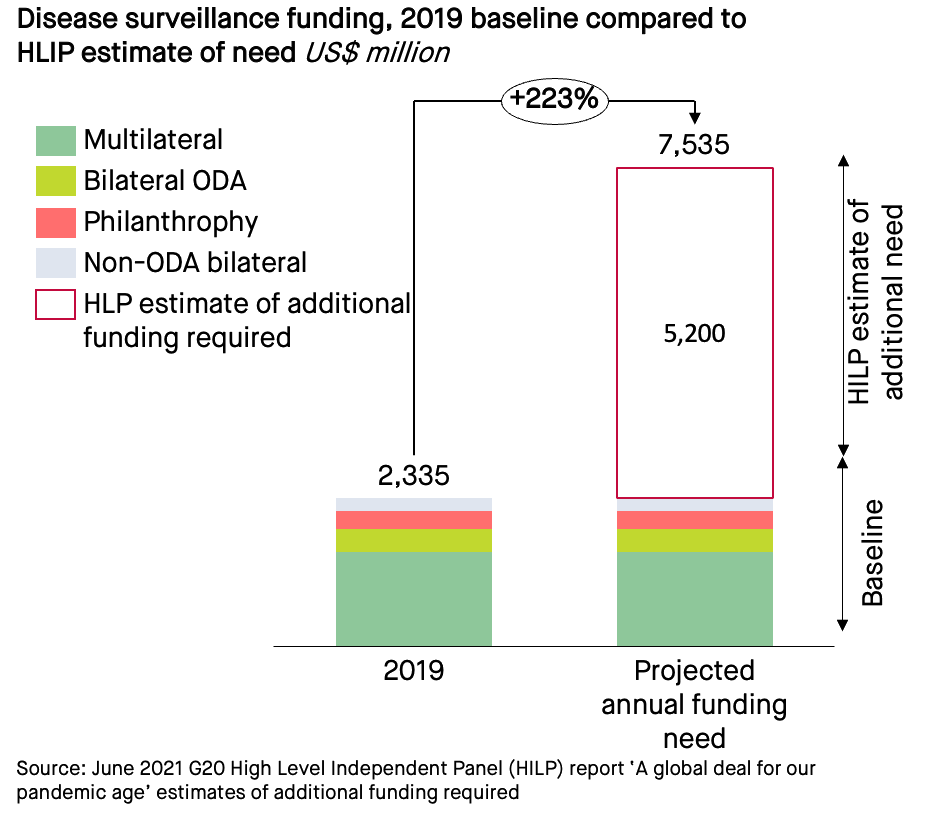
International funding needs to be scaled up significantly to meet the G20 HLIP target
The G20 HLIP called for additional disease surveillance funding - an additional US$5.2 billion per year over five years above 2019 and 2020 estimates. To meet the additional need identified by the G20, international funding for disease surveillance would need to increase more than threefold from a 2019 baseline. Even the significantly increased 2020 funding levels for disease surveillance are far below what is needed to adequately prevent and detect emerging infectious diseases. The emergency nature of these uses and sources of funding during 2020 suggests that there is a significant risk that funding may revert to the baseline level once the COVID-19 crisis is considered ‘over’.
Domestic disease surveillance funding is inadequate to respond to future outbreaks
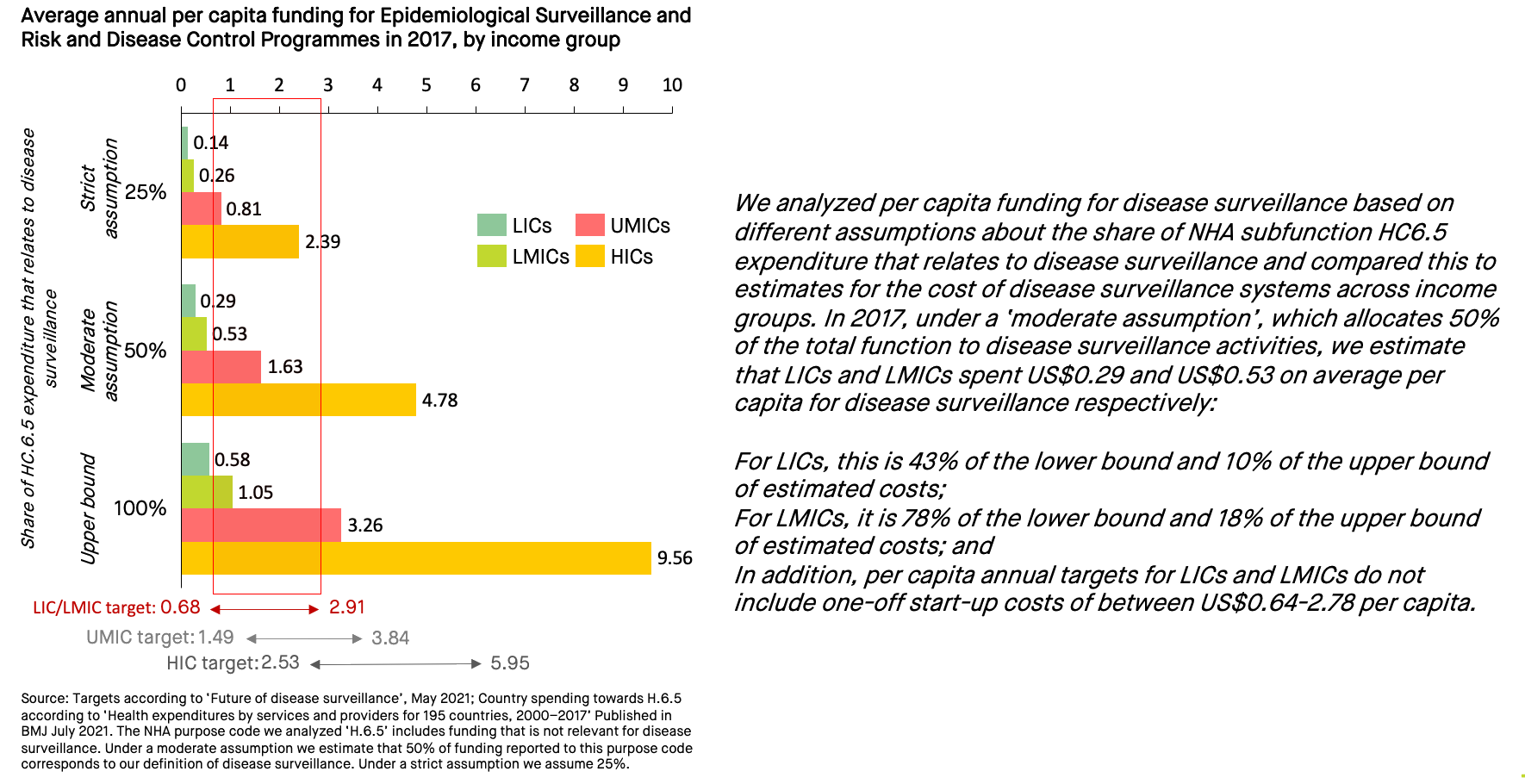
Information on domestic level funding for disease surveillance is scarce and inconsistent. Despite limited data, we know that funding at the domestic level for disease surveillance is extremely low, especially in low-income countries (LICs) and lower-middle-income countries (LMICs). Tracking this funding is difficult because country-level reporting is irregular, and the data are not granular enough to specifically measure disease surveillance funding.
The National Health Accounts (NHA) data provides the best estimates available for country-level spending. Examining subfunction HC6.5, Epidemiological Surveillance and Risk and Disease Control Programmes (subfunction HC.6.5), while including far more than just disease surveillance spending, gives us a range within which we can estimate domestic level spending on disease surveillance. The data demonstrates significant underspending in LICs and LMICs compared to both high-income countries (HICs) and the G20 HLIP target.
International funders and HICs should ramp up funding for LICs and LMICs for domestic disease surveillance capacities. While more international funding is necessary on the domestic level for LICs and LMICs, in-country capacity for disease surveillance would need to be scaled up in tandem to increase individual countries’ ability to absorb international funding.
Nexts steps on disease surveillance
While the COVID-19 pandemic exposed challenges in disease surveillance, it also intensified efforts to fill the gaps, leading to new investments at the national and global levels. Momentum in the wake of COVID-19 should be maintained to ensure that shortcomings are addressed appropriately, and additional funding is mobilized. To improve disease surveillance systems, advocates, governments, and multilaterals need to ‘scale, integrate, and track’.
- Scale-up funding for disease surveillance International public and private financiers need to triple their investments in integrated disease surveillance to achieve the goals set out by the G20 HLIP.
- Increases in funding sourced from emergency budgets in 2020 should be translated into sustained funding streams. The Global Fund’s replenishment in 2022 is one of many opportunities to make sustained increases in funding for disease surveillance a priority;
- The Financial Intermediary Fund (FIF) for Pandemic Prevention, Preparedness, and Response (PPR), hosted by the World Bank, should prioritize integrated disease surveillance and become an engine for more integrated, scaled-up financing; and
- Advocates should emphasize funding for integrated disease surveillance as a foundation for all health priorities. While recent attention to disease surveillance comes from a pandemic preparedness perspective, the benefits of investing in integrated disease surveillance are much broader and should be emphasized as part of a campaign to increase international and domestic funding for disease surveillance.
- Integrate funding for disease surveillance Additional international funding should be channeled through the multilateral system, as it is the most efficient way to support countries in building integrated disease surveillance systems.
- Additional funding should capitalize on and complement existing multilateral mechanisms already funding disease surveillance– most notably at WHO, the Global Fund, and the World Bank. This is consistent with the World Bank’s recent proposals for the FIF.
- Existing international funding for disease surveillance must be better integrated to deliver broader health system benefits and to reduce inefficiencies and barriers to impact. Supporting the development of fully integrated disease surveillance models in select countries should be a priority for financial and technical assistance.
- Major public and private funders of disease surveillance should agree on pathways for aligning disease surveillance funding, such as through the adoption of global standards (e.g., on data collection or survey protocols); and
- International funders should work with exemplar countries to understand and demonstrate the value of and approaches to integrating funding for disease surveillance at the country level. They should provide targeted funding and capacity building to national public health institutes to collect, connect, analyze, and act on disease surveillance data.
- Track funding for disease surveillance The international community needs to agree upon a common definition and framework for disease surveillance to support the development of a targeted strategy for scaling up and integrating funding.
- Major funders could convene to align on and widely accept a working definition of disease surveillance that can be used to track funding.
- Ongoing tracking of funding for disease surveillance should be instituted based on this common definition to increase transparency and accountability of international and domestic funding for disease surveillance.
- International actors could convene a task force to agree on a shared methodology for tracking and reporting funding for disease surveillance (e.g., using a Muskoka-like approach). This tracking could be tied to wider accountability efforts to increase international and domestic funding for PPR; and
- International funders and multilaterals could encourage the OECD DAC to collect comparable information on international funding for disease surveillance and institute annual reporting to promote transparency around funding for disease surveillance.
By scaling up, integrating, and tracking disease surveillance funding, advocates, public and private financiers, and governments will be better prepared to respond to the next pandemic and support more robust health systems overall.
Notes
The OECD’s dataset on Official Development Assistance (ODA) is not set up to track cross-cutting flows to topics such as disease surveillance. Many of the multilateral and philanthropic organizations we interviewed had no centralized overview of their disease surveillance activities or funding. At a domestic level, there is no comparable national tracking of funding for disease surveillance systems.
Further Readings
International Health Regulations - WHO
Interested in commissioning analysis in financing or development tailored for your organization’s specific needs?
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.

Emily Wymer

Sinéad Dwyer
Related Publications
Be the first to know. Get the latest in development news, right in your inbox.
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.
By clicking Sign Up you're confirming that you agree with our Terms and Conditions .
an initiative by SEEK Development
SEEK Development
The Donor Tracker is an initiative by SEEK DevelopmentContact
SEEK DevelopmentCotheniusstrasse 310407 BerlinGermany